Digital Competence Lab (DCL) for Speech Therapy |
Designing a learning platform to advance digital skills
| Journal | Industry 4.0 Science |
| Issue | Volume 42, 2026, Edition 1, Pages 110-118 |
| Open Access | https://doi.org/10.30844/I4SE.26.1.102 |
| Bibliography | Share | Cite | Download |
Abstract
Keywords
Article
Digital transformation and role change in speech therapy
The ongoing digitalization of healthcare is reshaping speech therapy services [1]. At the same time, the demands placed on professionals are increasing: speech therapists must not only be able to use digital tools competently, but also critically evaluate their benefits, integrate them into therapy in an evidence-based manner, and provide informed advice to patients and their families. This development is thus broadening the role of speech therapists – beyond traditional therapy, they are increasingly taking on evaluative and advisory tasks [3].
Against this backdrop, digital competence development is becoming a central concern. Our understanding of competence follows an expanded, profession-related perspective that encompasses technical, reflective, and communicative dimensions [15, 16]. Digital competence therefore does not simply refer to the ability to operate individual tools, but to the evidence-based evaluation of technologies, their responsible integration into therapeutic processes, and to the ability to advice patients and families in a target-group-appropriate manner . Digital competence is thus understood as a dynamic interplay of knowledge, skills, and attitudes that must be developed in context-specific ways and continuously refined [3].
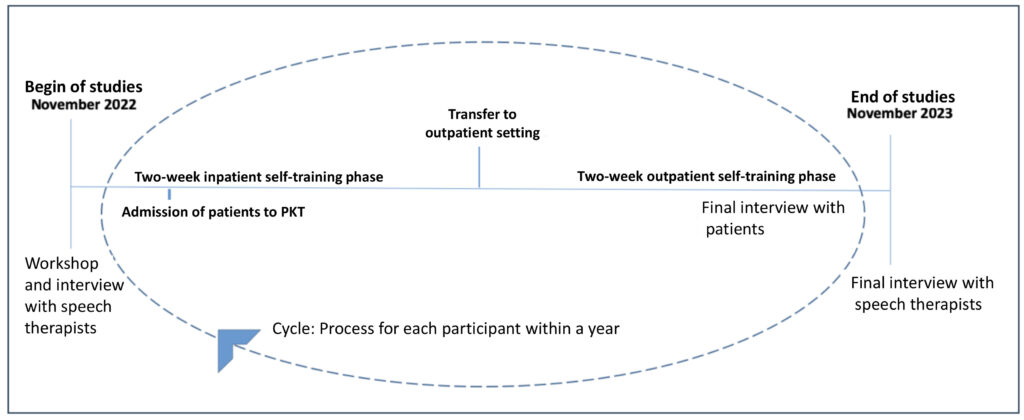
Within the framework of the HUMAINE Competence Center, AI-supported applications, in particular the AI-based application ISi-Speech-Sprechen, were examined in a feasibility study in the context of Parkinson’s complex therapy (PKT) (Figure 1).
The results indicate clear potential, including a higher exercise frequency and increased motivation among patients. At the same time, they reveal a greater need for consultation, technical challenges, and a strong need for digital competence among therapists. The Digital Competence Lab (DCL) was developed as a structural response to these challenges.
The DCL is a web-based, competence-oriented learning and implementation platform for speech therapists that bundles modular, practice-oriented offerings to support the development of digital skills. The platform aims to systematically translate research findings into speech therapy practice, promote digital skills, and support the sustainable integration of smart technologies such as AI. The aim of this article is therefore to
- outline the digital transformation of speech therapy and the resulting need for digital skills
- derive key dimensions of work design in the context of smart technologies based on the ISi-Speech-Sprechen use case
- conceptually and critically examine the DCL as a practice-oriented, competence-focused implementation platform
The focus is therefore on how speech therapists can systematically develop digital skills in order to implement AI-supported tools such as ISi-Speech-Sprechen in routine speech therapy care over the long term.
Digitization of speech therapy: opportunities and challenges
Digital transformation affects not only technical infrastructures but also organization, education, and care [1]. In speech therapy, digital tools offer a wide range of possibilities: speech-supporting apps, digital home-exercise tools, and AI-based feedback systems can complement face-to-face therapy [2]. At the same time, considerable structural challenges persist. In Germany, approximately 30,000 speech therapists serve a growing number of patients with speech and language disorders [5]. Shortages of skilled professionals, long waiting times for therapy places, and high administrative burdens complicate care delivery [6, 7, 8, 9]; the profession was already classified as a shortage occupation in 2018 [7].
In addition to structural factors, identity- and profession-related aspects are central Speech therapy has traditionally been characterized by personal interaction, therapeutic relationships, and individualized treatment approaches [3]. The introduction of digital technologies therefore raises professional and ethical questions – especially when AI systems affect core diagnostic or therapeutic areas and shift activities that have previously been integral to professional expertise [10].
This context emphasises the growing importance of digital skills. These include not only technical knowledge, but also the ability to evaluate technologies in an evidence-based manner, use them responsibly, and provide guidance to patients [11, 12]. The development of such skills is increasingly viewed as a professional ethical obligation [13, 14].
Nevertheless, digital content has not yet been systematically integrated into education, training, and continuing education [15, 16]. International studies indicate that targeted skills development is crucial for the successful implementation of telehealth formats and AI-based tools [32]. This highlights the need to structurally embed digital skills development within speech therapy and to support it through practical training formats – this is where the DCL comes in.
Use case: AI-supported dysarthria therapy with ISi-Speech-Sprechen
A key area of application for digital therapy supplements is the treatment of dysarthria in Parkinson’s disease. Up to 89% of those affected develop speech motor impairments over the course of the disease, manifested in reduced speech volume, monotonous prosody, and decreased intelligibility [17, 34]. Clinical guidelines for neurological speech and language disorders recommend high-frequency, individualized therapy sessions; however, these recommendations are often difficult to implement in routine care settings[17].
In the HUMAINE research project, the AI-based application ISi-Speech-Sprechen served as an exemplary use case for smart AI technologies in speech therapy [19, 20]. The web-based, AI-supported app includes over 2,500 evidence-based exercises on articulation, prosody, speech volume, speech rate, voice volume, and respiration. Using automatic speech recognition, the system analyzes patients’ speech performance and generates AI-based feedback to support individualized training control. Unlike existing digital training systems (e.g., LSVT Coach), which are based on proven methods [18], ISi-Speech-Sprechen also integrates AI-supported analysis and feedback mechanisms to further individualize self-training [18, 19, 20].
Focus group interviews with speech therapists were conducted to gather professional perspectives [22, 23]. Participants emphasized the need for continuous skills development, discussed tensions between new technologies and traditional professional identities, and pointed to framework conditions such as limited time resources, inadequate technical equipment, and existing remuneration structures. Building on these insights, a feasibility study was designed in the real-world setting of complex Parkinson’s therapy (PKT). In this study, patients with Parkinson’s- related dysarthria trained independently with ISi-Speech-Sprechen over several weeks in addition to face-to-face therapy.
The detailed results of this study are reported in the original article. For the purposes of the present article, the most relevant results are those that highlight implications for competence development and work design: increased exercise frequency and high user acceptance, increased need for advice and support, technical challenges in everyday practice, and the necessity of systematically building digital skills to enable therapists to safely guide patients. These findings also mark the starting point for the design of the Digital Competence Lab (DCL) as a transfer and development platform to promote digital skills among speech therapists.
Challenges in implementing smart technologies
The introduction of digital applications such as ISi-Speech-Sprechen illustrates that technological innovation alone is insufficient. Successful implementation requires a context-sensitive approach that gives equal consideration to technical, professional, organizational, and ethical dimensions [25, 26]. From a technical perspective, infrastructure, data protection, and IT support are key prerequisites. Professionally, smart technologies are reshaping role profiles and competence requirements: speech-language pathologists are increasingly assuming consulting and evaluation tasks that go beyond traditional therapeutic activities [30, 31].
Organizationally, a key challenge is to integrate new applications into heterogeneous care settings, ranging from outpatient practices to inpatient facilities [33]. This challenge is further compounded by the heterogeneity of education and training pathways. Different qualification routes are accompanied by varying curricula and levels of digital content, which requires needs-based implementation and tailored qualification strategies.
Ethical considerations also play a central role, particularly with regard to responsibility, transparency, and relationship building. Questions arise as to how therapeutic interactions change when AI-supported systems generate feedback that was previously provided by professionals [10]?
Another key problem to remain is the so-called translation gap, whereby many technological innovations do not make it into healthcare practice [21]. To close this gap, the early involvement of speech-language pathologists and suitable structures to promote digital competence development are crucial. Findings from the HUMAINE project underscore that implementation processes can only succeed when technical and professional perspectives are systematically linked. This insight forms the basis for the development of the DCL, which is discussed below as a structural response to the identified requirements.
Core aspects of work design
Findings from the needs analysis and feasibility study show that integrating smart technologies not only requires technical adjustments but also has a profound impact on the design of speech therapy work. Five dimensions emerged as particularly relevant: capacity to act and competence development, augmentation and workload relief, role development, participation and context specificity, and organizational development. These dimensions provide the framework for the design of the DCL. Accordingly, the learning opportunities within the DCL are aligned with these perspectives to closely link competence development to real-world work requirements.
Capacity for action and competence development
Speech therapists must be able to use technological applications, critically evaluate their benefits, integrate them into therapy planning in an evidence-based manner, and advise patients and their families. This results in a dual function: acting both as users of smart technologies and as mediators within the care context. Continuous competence development is therefore a prerequisite for professional, confident practice and simultaneously strengthens therapist’s ability to actively shape digital transformation processes [36].
Digital competence encompasses technical, reflective, and communicative skills that must be systematically developed and updated in everyday professional practice. The DCL explicitly addresses this cycle: competence acquisition → reflective selection → context-sensitive implementation → evaluation [15, 16]. Concrete learning elements such as case studies, decision-making tasks, and reflection prompts on implementation scenarios are designed to support the transfer of newly acquired competencies into therapist’s own fields of work.
Augmentation and workload relief
AI systems can increase the flexibility of speech therapy processes. By supplementing face-to-face therapy with digital self-training with individualized feedback, the number of weekly sessions can increase significantly [19]. In the feasibility study on ISi-Speech-Sprechen, patients completed an average of four additional AI-supported sessions of 20 minutes per week (range 1–7), in addition to face-to-face therapy. Therapists reported a sense of relief, as the application enabled care beyond the therapy sessions and enhanced patient motivation and adherence:
“I noticed that my patients who simultaneously worked with the app were significantly more motivated in the face-to-face therapy itself … this had a direct impact on the overall therapy.” (Interview t3, therapist 1, pos. 6)
In addition to therapeutic content, AI applications offer potential for reducing administrative burdens (e.g., appointment and resource planning, documentation, evaluation of speech diagnostic data). Furthermore, AI-supported training can enable patients to practice more effectively and independently.
Adaptive exercise formats and individualized feedback strengthen self-efficacy and personal responsibility, thereby reducing the workload for professionals and strengthening the patient’s active role in the long term [19, 32]. The DCL addresses these aspects, among other things, through tutorials on designing digitally supplemented therapy settings and guidelines for patient counseling.
Role development
The introduction of smart technologies is reshaping professional roles and areas of responsibility. Therapists are taking on a dual role as users of digital systems and as advisors who guide patients, answer technical questions, and recommend suitable applications [32, 1]. This expands the professional profile toward that of a “smart therapist.” One interview participant described this shift as follows:
“Since we already have a certain advisory function and recommend other tools or therapies, this is basically just another point – we already have the advisory role anyway.” (Interview t1, therapist 1, pos. 96)
This shift in roles requires adjustments in training, qualification profiles, and continuing education and training [30, 31]. The DCL responds to these needs by addressing changing roles and providing spaces for reflection.
Participation and context specificity
The successful integration of AI-based systems depends on the early, active involvement of professionals – especially in the design, implementation, and optimization processes. Speech therapy practice is contextually diverse (outpatient practices, interdisciplinary centers, inpatient care). Different infrastructures, patient profiles, and training levels require context-sensitive strategies [26]. Universal “all-in-one solutions” have proven not to be realistic. Instead, smart tools must be adapted to local conditions. Implementation decisions should consider suitability, technical affinity, and cost-benefit ratio. The DCL supports context-sensitive competence development by integrating experience reports, case studies, and design recommendations tailored todifferent care settings.
Organizational development
At the organizational level, digital solutions can support practice management, documentation, scheduling, and communication, thereby freeing up resources for patient-centered care [33]. In structurally underserved regions, the targeted use of digital applications can help address gaps in care and strengthen therapeutic continuity. Quality-assured digital additions can improve accessibility, efficiency, and participation; smart technologies thus also contribute to broader health policy objectives such as inclusion, equal opportunities, and sustainability [4, 25].
The DCL addresses this level through materials on infrastructure and data protection requirements, as well as examples of practice and clinic processes that systematically integrate the use of smart technologies.
The Digital Competence Lab (DCL)
Findings from HUMAINE and the feasibility study on ISi-Speech-Sprechen indicate that the successful use of AI-supported applications depends not only on technical functionality, but also on digital competence. This includes technical, reflective, and advisory skills that must be systematically developed, applied, and continuously refined. The DCL was developed as a structural response to these requirements.
Theoretical and didactic foundations of the DCL
Digital competence is understood as the ability to (1) understand digital technologies on a sound technical basis, (2) critically evaluate them, (3) integrate them responsibly and in a patient-oriented manner, and (4) communicate them in a way that is appropriate to the target audience. The DCL is based on established reference frameworks for digital competence [15, 16, 38]. The content structure (including video tutorials, podcasts, data protection materials, curated literature database) and navigation are based on the European reference framework for digital competences (DigComp) and the framework “Competences in the Digital World” [15, 16, 38].
In terms of didactics, the DCL follows principles of goal- and competence-oriented learning, problem relevance, clear structuring, activation/self-efficacy, differentiation, and target group orientation [16, 26, 36, 39]. The content is based on real-life requirements from research, practice, and implementation and is presented in micro-structured learning units that contain tasks, examples, and prompts for reflection.
In terms of media didactics, the DCL builds on principles of multimedia learning (e.g., coherence, segmentation, and contiguity principles) as well as on design principles of user-centered, barrier-free learning environments [39, 40, 41, 42]. As a dynamic platform, the DCL is designed in such a way that content and formats can be continuously adapted to new developments and requirements.
Structure and design elements
The DCL is a multi-perspective implementation and learning platform that combines scientific, practical, and professional policy perspectives.
It offers, among other things:
- step-by-step tutorials for the introduction and use of specific digital tools across different care settings
- podcasts featuring experts from research, clinical practice, and development, as well as representatives from other health professions
- materials to support patient counseling (e.g., informational materials, checklists)
- modules for digital competence development (basics of AI, data security, ethical considerations, implementation strategies), illustrated with speech therapy-specific examples
- planned reflection and self-assessment elements to support the evaluation of skill levels and attitudes and to identify areas for further development
All content is accessible independent of time and location and can be integrated into everyday clinical work in a resource-efficient manner. The platform also functions as an open development and networking environment in which speech-language pathologists can contribute their experiences, comment on content, and contribute to its ongoing development.
Contribution to role development and practice design
The DCL is designed not merely as a platform for imparting technical knowledge, but as a tool for strengthening professional capacity for action in digitized care settings. Case-based learning opportunities, consultation guidelines, and interaction scenarios support the ongoing development of professional roles toward that of “smart therapists”, combining therapeutic, technical, and consulting expertise.
At the same time, the DCL addresses organizational and context-specific issues (e.g., embedding digital applications in practice processes, interprofessional coordination, documentation). In doing so, the platform supports a reflective and responsible approach to digitalization that is grounded in transparency, participation, inclusion, and accessibility[26, 36]. The DCL acts as a bridge between research, education, and healthcare practice, thereby supporting responsible knowledge transfer.
Critical reflection and perspectives for further development
The DCL is intentionally conceived as an open and evolving platform that must be continuously adapted to changing technological, professional, and organizational conditions. Several challenges emerge in this context. These include heterogeneous educational pathways and varying levels of prior digital experience among speech therapists, limited time resources for continuing professional development, differences in technical infrastructure across care settings, and the need to regularly update content in response to rapid technological advances.
In addition, consideration must be given to how digital learning formats are designed to ensure that inequalities in digital participation are not exacerbated. Participatory further development and close links with professional associations, educational institutions, and care providers are central to this process.
Further evaluations should examine the extent to which DCL use is associated with measurable improvements in digital skills (e.g., pre-post measurements, skills tests, self-assessment, and external assessment) and how this affects implementation processes and care outcomes. Such studies could provide evidence of effectiveness and inform targeted further developments.
Discussion and outlook
Based on the results of the feasibility study on ISi-Speech-Sprechen in Parkinson’s complex therapy (PKT) outlined in this article, it is clear that AI-supported systems can meaningfully enhance therapeutic interventions in speech therapy – for example, through increased exercise frequency, individualized feedback, and increased patient motivation – but at the same time pose structural, organizational, and competence-related challenges [19, 27, 28, 29]. Due to the small sample size and the specific setting, these results cannot be generalized; rather, they serve as an exemplary starting point for identifying key dimensions of work design in the context of smart technologies and deriving requirements for the systematic development of digital competencies.
From this perspective, the ISi-Speech-Sprechen use case functions as an analytical lens that reveals the areas of tension between new technologies, existing healthcare realities, and professional identity. Against this backdrop, the DCL is designed as a structured response to these challenges. Its focus on problem-oriented learning approaches, blended learning formats, and reflective elements supports an understanding of digital technologies not only as additional specialist knowledge, but as an integral part of professional practice. This shifts the focus away from whether speech-language pathologists should use digital tools toward how they can do so competently, reflectively, and in a context-specific manner.
At the same time, it is evident that, despite these strengths, the DCL faces several conceptual and practical limitations. While its alignment with overarching competency frameworks enables a high degree of compatibility with educational and health policy discourses, it also entails the risk that speech therapy–specific characteristics and context-dependent requirements may not be sufficiently reflected.
In addition, the strong emphasis on self-directed and digitally supported learning processes requires a minimum level of media literacy, time resources, and institutional support. Without the appropriate structural conditions – such as reliable time resources for continuing education and training or adequate technical infrastructure – there is a risk that primarily digitally proficient professionals will benefit from the DCL, while existing inequalities in digital participation will be exacerbated rather than reduced [25, 26, 36].
Another critical aspect concerns the reach and representativeness of the DCL. The platform was designed with a specific field of application (AI-supported dysarthria therapy for Parkinson’s disease) and a clearly defined care structure (PKT) in mind. Whether, and to what extent, the learning modules, scenarios, and materials can be transferred to other disorders, care contexts, and qualification paths remains to be seen. This highlights the need to further modularize the DCL, expand it in a context-specific manner, and supplement it with additional use cases from speech therapy practice in order to adequately reflect the heterogeneity of the field.
Closely linked to this is the challenge of continuously updating content in the face of rapid technological developments while ensuring sufficient didactic quality assurance. From an evaluative perspective, there is a clear need to systematically assess the contribution of the DCL to the digital professionalization of speech therapy. This calls for multi-stage study designs that record changes in digital action skills before and after the use of selected DCL modules, analyze correlations between DCL use, implementation success, and patient outcomes, and explore speech therapists’ qualitative experiences with the platform in terms of role development, self-efficacy, and ethical reflection.
In addition, evaluation approaches that iteratively further develop DCL learning offerings in collaboration with users, in line with principles of human-centered design, appear particularly promising.
Furthermore, international networking with comparable initiatives in the field of digital learning platforms and competence development in healthcare is recommended in order to leverage synergies, exchange examples of good practice, and develop shared standards for digital competence profiles in speech therapy over the longer term. Such collaboration could not only support the continued development of the DCL in terms of content and structure, but also strengthen its integration into international discourses on digital health education.
Overall, this article suggests that the DCL—when combined with structural measures in education, training, and continuing professional development—has the potential to make a substantial contribution to the digital professionalization of speech-language pathology and to prepare the discipline for the demands of increasingly technology-supported, human-centered healthcare. At the same time, a sustainable impact can only be expected if the platform is understood as an evolving learning structure and accompanied by rigorous empirical research. By integrating technological innovation, ethical reflection, and practical applicability, the DCL provides a foundation for a sustainable, participatory, and responsible approach to digital transformation in speech-language pathology.
The original German version of this article can be accessed via DOI: 10.30844/I4SD.26.1.110
Bibliography
[1] Leinweber, J. (2023). Digitale Transformation in der Logopädie. Gesundheitsberufe im Wandel, 4(2), 22–30.[2] Ritterfeld, U., & Hastall, M. (2017). Smarte Technologien zur Förderung von Sprache und Teilhabe. In Digitale Medien in der Gesundheitsförderung (S. 101–118). Springer.
[3] Berretta, S. (2024). Job-Identität im Wandel: Erfassung der beruflichen Identifikation und Bedrohung dieser durch den Einsatz von KI in der Logopädie und Beratung. AOW Newsletter Komplexität & Lernen, (70), 16–18.
[4] Duval, S., Diederich, N., & Defer, G. (2018). Versorgungslücken bei Parkinson-Patienten mit Sprachstörungen. Journal für Neurologie, 265(7), 1073–1080.
[5] opta data Institut. (2022). 4. Statistisches Jahrbuch zur gesundheitsfachberuflichen Lage in Deutschland 2022 – Heilmittel. opta data Institut für Forschung und Entwicklung im Gesundheitswesen e. V.
[6] Thissen, S. (2019). Lilien kann nicht richtig sprechen – doch auf Hilfe muss die Sechsjährige ein halbes Jahr warten. Stern. https://www.stern.de/gesundheit/logopaeden-am-limit–ein-besuch-in-einer-praxis-in-hamburg-8636950.html
[7] Bundesagentur für Arbeit. (2021). Fachkräfteengpassanalyse 2021. In Statistik/Arbeitsmarktberichterstattung (Hrsg.), Berichte: Blickpunkt Arbeitsmarkt. https://www.vbw-bayern.de/Redaktion/Frei-zugaengliche-Medien/Abteilungen-GS/Bildung/2022/Downloads/Engpassanalyse-2021.pdf
[8] Schwarzmann, A.-L., Gerlach, S., Rohde-Schweizer, R., Straßer, B., Paul, S., & Hammer, S. (2018). „Ich bin dann mal weg!“ – Eine Studie zur Berufsflucht von Logopäd*innen. Forum Logopädie, 32(3), 22–27.
[9] Pula-Keuneke, A. (2021). Befragung logopädischer Praxen in Hessen zeigt schwierige Versorgungslage auf. Deutscher Bundesverband für Logopädie e. V. https://www.dbl-ev.de/service/meldungen/meldung/befragung-logopaedischer-praxen-in-hessen-zeigt-schwierige-versorgungslage-auf
[10] Ehlert, H., & Lüdtke, U. (2023). Künstliche Intelligenz (KI) in der Logopädie: Potenzial und Herausforderungen am Beispiel einer Automatisierung der Diagnostik im Bereich Kindersprache. forum:logopädie, 37(6), 6–11.
[11] Alber, B., & Starke, A. (2021). Digitale Kompetenzen von Sprachtherapeut*innen – Therapieren (DiKoST-T). Forschung Sprache, 9(2), 3–11.
[12] Starke, A., Leinweber, J., & Ritterfeld, U. (2016). Neue Medien in Therapie und Unterricht für Kinder mit dem Förderschwerpunkt Sprache. Praxis Sprache, (1), 28–32.
[13] Euben, D. (2020). Top 10 Ethical Considerations in Using Telepractice. https://leader.pubs.asha.org/do/10.1044/2020-0513-ethics-telepractice/full/
[14] Leinweber, J., & Schulz, K. (2019). Digitalisierung in der Aphasietherapie – eine ethische Betrachtung. Aphasie und verwandte Gebiete, 46, 34–41.
[15] Kultusministerkonferenz (KMK). (2017). Strategie der Kultusministerkonferenz „Bildung in der digitalen Welt“. Beschluss vom 8.12.2016 in der Fassung vom 7.12.2017. https://www.kmk.org/fileadmin/pdf/PresseUndAktuelles/2018/Digitalstrategie_2017_mit_Weiterbildung.pdf
[16] Leinweber, J., & Dockweiler, C. (2020). Digitale Kompetenzentwicklung im Gesundheitswesen. In C. Dockweiler (Hrsg.), Digitale Transformation in Gesundheitsberufen (S. 51–72). Beltz Juventa.
[17] Ackermann, H., et al. (2018). Neurogene Sprechstörungen (Dysarthrien), S1-Leitlinie. In Deutsche Gesellschaft für Neurologie (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie. https://www.dgn.org/leitlinien(abgerufen am 12.06.2025)
[18] LSVT Global. (2016). LSVT LOUD Clinician’s Guide. LSVT Global Inc.
[19] Frieg, H., Mühlhaus, J., Ritterfeld, U., & Bilda, K. (2017). Assistive Technologien in der Dysarthrietherapie: Entwicklung des Trainingssystems ISi-Speech als Anwendungsbeispiel. Forum Logopädie, 31(3), 10–15.
[20] Ritterfeld, U., Mühlhaus, J., Frieg, H., & Bilda, K. (2016). Developing a technology-based speech intervention for acquired dysarthria: A psychological approach. In K. Miesenberger, C. Bühler, & P. Penaz (Eds.), ICCHP 2016, Part I, Lecture Notes in Computer Science, 9758 (S. 93–100). Springer.
[21] Shaw, J., Rudzicz, F., Jamieson, T., & Goldfarb, A. (2019). Artificial intelligence and the implementation challenge. Journal of Medical Internet Research, 21(7), e13659.
[22] Bilda, K., Dörr, F., & Thurmann, A. (2022). Artificial intelligence solutions in Parkinson therapy. In T. Ahram, W. Karwowski, P. Di Bucchianico, R. Taiar, L. Casarotto, & P. Costa (Eds.), Intelligent Human Systems Integration (IHSI 2022): Proceedings of the 5th Conference on Intelligent Human Systems Integration. AHFE International Open Access.
[23] Bilda, K., Thurmann, A., & Dörr, F. (2023, 31. Mai–2. Juni). Artificial intelligence in routine speech therapy care for Parkinson’s disease. Development of a human-centered implementation approach. Fourth International Congress on Neurorehabilitation and Neural Repair, Maastricht, Netherlands.
[24] Scherbaum, R., Höllerhage, M., Klebe, S., Riederer, P., Müller, T., Schröter, N., Weise, D., Woitalla, D., & Tönges, L. (2025). Parkinson’s Disease Multidisciplinary Complex Therapy (PD-MCT): Appreciation of its current function for the treatment of people with Parkinson’s disease in Germany and the needs of future development. Journal of Neural Transmission. Advance online publication.
[25] Steiner, L. (2023). Digitale Teilhabe in der Logopädie: Einstellungen, Kompetenzen und Herausforderungen. Zeitschrift für Sprache & Kommunikation, 48(1), 37–50.
[26] Beres, A., Schäfer, A., & Neff, D. (2019). Human-Centered Design in digitalen Gesundheitstechnologien. Springer.
[27] Jakob, H., Pfab, J., Prams, A., Ziegler, W., & Späth, M. (2022). Digitales Eigentraining bei Aphasie: Real-World-Data-Analyse von 797 Nutzer*innen der App »neolexon Aphasie«. Neurologie & Rehabilitation, 28, 61–67.
[28] Ziegler, W. (2012). Rehabilitation aphasischer Störungen nach Schlaganfall. In H. C. Diener & C. Weimar (Hrsg.), Leitlinien für Diagnostik und Therapie in der Neurologie (S. 1087–1095). Thieme.
[29] Korsukewitz, C., et al. (2013). Wieder richtig sprechen lernen. Ärztliche Praxis Neurologie Psychiatrie, 4, 24–26.
[30] Langholf, V., & Wilkens, U. (2024). Pathway to work with AI: Testing the clAIr role development method in an industrial work environment. Zeitschrift für Arbeitswissenschaft, 78, 377–386.
[31] Berretta, S., Tausch, A., Kluge, A., & Peifer, C. (2023). The Job Perception Inventory: Considering human factors and needs in the design of human-AI work. Frontiers in Psychology, 14, 1128945.
[32] Wade, V. A., Eliott, J. A., & Hiller, J. E. (2014). Clinician acceptance is the key factor for sustainable telehealth services. Qualitative Health Research, 24, 682–694.
[33] Matusiewicz, D. (2023). Künstliche Intelligenz im Gesundheitswesen. In Gesundheit 5.0 – Digital und patientenzentriert (S. 85–98). medhochzwei Verlag.
[34] Ackermann, H., Ziegler, W., & Vogel, M. (2018). Dysarthrie bei Parkinson: Diagnostik und Therapie. Sprache · Stimme · Gehör, 42(1), 1–9.
[35] Frieg, H., Mühlhaus, J., Ritterfeld, U., & Bilda, K. (2017). Assistive Technologien in der Dysarthrietherapie. Forum Logopädie, 31(3), 10–15.
[36] Leinweber, J., & Dockweiler, C. (2020). Perspektiven der Digitalisierung in der Logopädie/Sprachtherapie. Ein Überblick über die Herausforderungen für Theorie, Forschung und Praxis. Forum Logopädie, 34(3), 6–9.
[37] National Institute on Deafness and Other Communication Disorders (NIDCD). (o. J.). Aphasia. https://www.nidcd.nih.gov/health/aphasia (abgerufen am 28.06.2025)
[38] Carretero, S., Vuorikari, R., & Punie, Y. (2017). DigComp 2.1: The digital competence framework for citizens with eight proficiency levels and examples of use. Publications Office of the European Union.
[39] Kerres, M. (2018). Mediendidaktik: Konzeption und Entwicklung digitaler Lernangebote (5. Aufl.). De Gruyter Oldenbourg.
[40] Mayer, R. E. (2009). Multimedia learning (2nd ed.). Cambridge University Press.
[41] Burgstahler, S. (Hrsg.). (2015). Universal design in higher education: From principles to practice (2nd ed.). Harvard Education Press.
[42] World Wide Web Consortium (W3C). (2018). Web Content Accessibility Guidelines (WCAG) 2.1. https://www.w3.org/TR/WCAG21/ (W3C).
Your downloads
Potentials: Innovation